October's Case of the Month - 2023
How Many Specialists Does It Take to Diagnose a Mass?
Patient Information:
Age: 3 years
Gender: Female (suspected spayed per rDVM)
Breed: Golden Retriever
Species: Canine
History:
Sandy was evaluated at her RDVM for weight loss, inappetence, and urinary incontinence on 5/11/2023. Exam revealed a large palpable mass on the right dorsocranial abdomen.
Ultrasonographic Findings:
Kidneys: Only the left kidney was readily visible. Enlarged size (Lt = 9.4 cm) and normal shape with normal corticomedullary dimensions. Moderate pyelectasia visualized (7.5 mm).
The right kidney appears severely hydronephrotic with minimally discernible septum creating a kidney-reminiscent shape, measured approximately 12.9 cm.
There is a heterogeneous, hyperechoic, peripherally vascular mass which appears to protrude into the area of the renal pelvis from the proximal ureter. Mass width exceeded the scope of the ultrasound probe (at least 9.4 cm), and mass depth is at least 8.7 cm.
Intestines: There is a focally mildly thickened segment of small intestine (max thickness 5.0 mm) with no sign of infiltrative disease.
Abdominal Ultrasound Interpretation:
Right hydronephrosis: The findings are severe—secondary to ureteral obstruction.
Right ureteral mass: The findings are severe. Differential diagnosis (Ddx): carcinoma (TCC/UC, other), soft tissue sarcoma, less likely granuloma.
Left Kidney Pyelectasia DDX:
- IV fluid administration
- Pyelonephritis and ureteritis
- Increased diuresis caused by renal insufficiency or other condition
- Toxin
- Infectious (leptospira, etc.)
- Post-renal obstruction / Bladder distention
- Diuresis
Images:

Image 1: Significant pyelectasia noted in the left renal pelvis.

Image 2: Hydrodronephrosis of the right kidney with soft tissue mass in the caudal pole suspected to be causing right ureter obstruction.
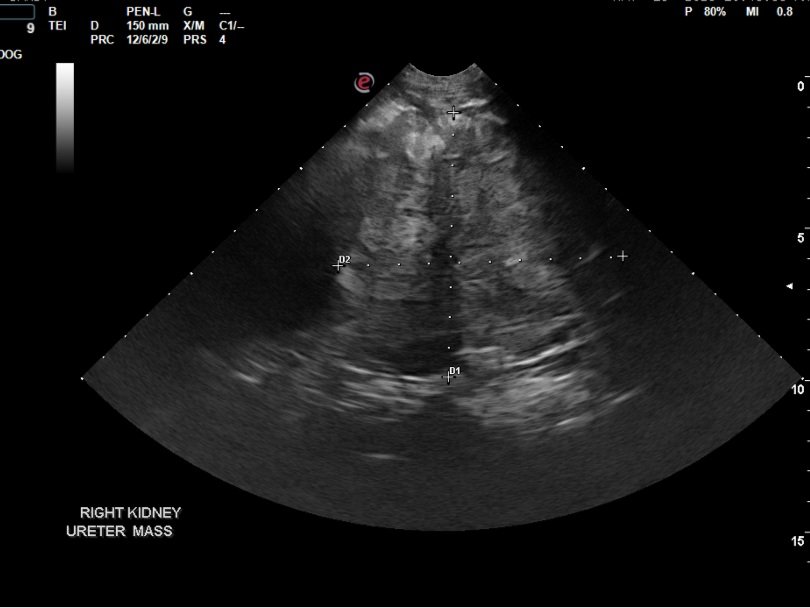
Image 3: Right caudolateral mass effect which extends beyond the scope of the ultrasound probe, located between the abnormal right kidney and cranial aspect of the urinary bladder.
Recommendations:
Referral to a veterinary surgeon for further diagnostics (CT scan, chest and abdomen) and therapy is highly recommended.
Additional Tests:
-
CT Scan:
- Variable but small volume fluid is noted in the peritoneal space.
- In the region of the right kidney, a large fluid-filled structure is identified with a soft tissue rim, thought to represent the renal capsule. It has a tubular extension medially and slightly caudally, thought to be the right ureter, which cannot be followed to the urinary bladder. This extends caudally to an approximately 11 cm x 8.5 cm irregularly marginated, soft tissue attenuating, heterogeneously enhancing, mildly complex mass located in the caudal abdomen to the right of midline, questionably retroperitoneal in location.
- Moderate left renal pelvic dilation is identified, tracing into a dilated left ureter which is mildly tortuous and also cannot be traced to the urinary bladder due to the large mass effect. This mass is displacing the caudal vena cava and associated more caudal branches dorsally, with compression. Invasion cannot be entirely excluded, especially caudal to the level of the renal parenchyma.
- The right renal vein is not specifically outlined. The aortic and additional sublumbar, including the medial iliac lymph nodes bilaterally, are variably enlarged although somewhat symmetrical.
- Both adrenal glands are difficult to specifically distinguish but are thought to be separate from this mass-like change and both are at least mildly enlarged.
- Conclusions: Large, more right-sided, complex soft tissue mass with regional peritoneal and retroperitoneal effusion. It is unclear if this represents a caudally positioned right kidney mass (less likely) or a caudal retroperitoneal cavitary mass with chronic ureteral obstruction, more severe on the right, leading to hydronephrosis and lack of renal parenchyma. More moderate to marked left pyelectasia to early hydronephrosis is identified with chronic partial obstruction from this mass. Neoplasia is the most likely cause, with hemangiosarcoma as a primary differential over round cell neoplasia or carcinoma. A right ureteral origin mass is not excluded but difficult to confirm due to the size and expansile appearance of the mass. Guided FNA may not provide additional information, and biopsy could be indicated. Surgical removal could be attempted, but involvement with the caudal vena cava and ureters cannot be specifically determined tomographically.

Photo: CT scanned image displaying the enormity of the mass used for surgical planning.
Surgery Report:
- Multiple firm, small, non-movable masses were present within the internal rectus sheath, inside the abdominal cavity.
- An extremely large, extensive, firm, and complex mass was present in the right mid to caudal abdomen, extending past midline adjacent to the pelvic brim. Upon further evaluation and careful dissection of some surrounding omental adhesions, the mass was found to be extremely complex and firm, with multiple organs adhered to or embedded within it, including the mid to distal duodenum, descending colon, right kidney, right ureter, uterine stump, apex of the urinary bladder, caudal vena cava, aorta, and femoral arteries.
- The right kidney was markedly distended, soft, and fluid-filled, resembling a large water balloon (approximately 12 cm in length). The mass measured an additional 9-10 cm in length and 8 cm in width.
- The segment of mid to distal duodenum, including the caudal duodenal flexure, was completely embedded within the mass and blocked the ability to discern the dorsal margin of the mass.
- Once the embedded duodenal segment was "removed," the dorsal and medial margins of the mass could be visualized. The caudal vena cava and aorta were noted cranially to the mass but were lost into the mass caudal to the left kidney. The mass appeared to have both a peritoneal and retroperitoneal component.
- A partial cystectomy was performed as the apical aspect of the urinary bladder and the distal uterine stump were completely embedded within the mass.
- The distal aspect of the right ureter was entering the urinary bladder, but the remaining proximal portion was completely embedded and lost into the mass. The mass also seemed firmly adhered to underlying epaxial musculature at the level of the mid-ureter.
- An additional extension of the mass was noted immediately dorsal to a segment of descending colon, which was deviated dorsally due to the mass. The sacral lymph node was visualized as enlarged and firm.
- Cytoreductive surgical removal of the most ventral aspect of the mass was performed. The interior of the mass appeared caseous and gritty, with a brown to white exudate. Approximately three-quarters of the mass was removed.

Photo 1: The excised bulk portion of the right abdominal mass which includes the right kidney, small intestines, colon, ureters and indiscriminate mesentery.
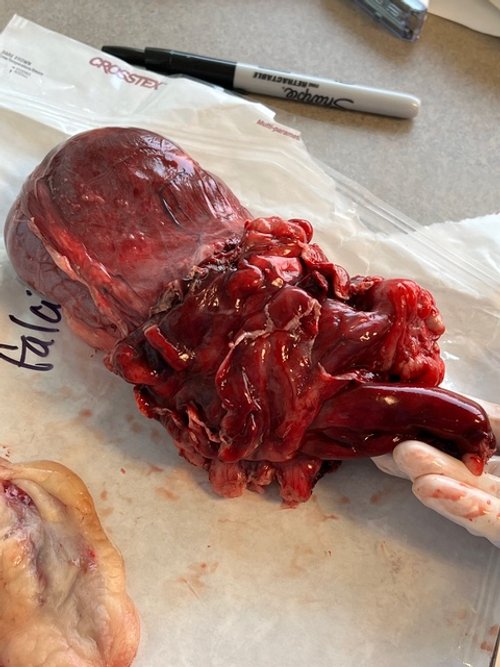
Photo 2: The excised bulk portion of the right abdominal mass, including the right kidney, small intestines, colon, ureters, and indiscriminate mesentery (slightly different angle).
Histopathology Report:
Pathological Findings, Diagnosis:
- Omental nodules: Severe, chronic, pyogranulomatous omentitis with suspected intralesional yeast or algae.
- Right retroperitoneal mass: Severe, chronic, pyogranulomatous retroperitonitis and nephritis with intralesional yeast or algae.
Comments:
- Both the omental nodules and the retroperitoneal mass were caused by severe, chronic, pyogranulomatous inflammation. Nodular inflammation often surrounded suspected yeast or algae (e.g., Prototheca). This inflammation and suspected organisms disrupted much of the kidney in the retroperitoneal sample. Further differentiation could not be performed due to negative staining with routine methods.
Microscopic Description:
- Omental nodules (slide A): Sections of omental fat showed nodules composed of dense macrophages mixed with neutrophils. Necrotic regions contained round, negatively staining fungal yeast or algal organisms (10–30 µm). Fibrosis, lymphocytes, plasma cells, edema, and hemorrhage were also noted.
- Right retroperitoneal mass (slides B1–B3): The retroperitoneal fat and kidney were infiltrated by severe nodular pyogranulomatous inflammation with necrotic regions containing yeast or algal organisms. Multinucleated cells and aggregates of lymphocytes and plasma cells were also present.
Discussion:
The genus Prototheca includes achlorophyllous, unicellular, saprophytic algae found in the environment. Protothecosis in dogs is rare but increasingly recognized. Unlike human cases, canine protothecosis is typically disseminated, affecting multiple organs, particularly the colon, nervous system, and eyes. Canine protothecosis often presents as chronic colitis and carries a grave prognosis, with most cases diagnosed at advanced stages. Early detection and understanding of the disease could improve outcomes.
Patient Outcome:
Immediate post-operative condition improved significantly, with increased activity, appetite, and comfort. Moderate regurgitation resolved with prokinetic therapy and nasogastric tube placement. The patient was discharged 48 hours post-surgery.
- At the 2-week recheck, significant improvements in comfort, activity, and demeanor were reported.
- Four months post-op, the patient was euthanized due to suspected recurrence of the growth and declining quality of life. Complete removal of abnormal tissue was not feasible during surgery.
Special thanks to Four County Animal Hospital for sharing patient details and Dr. Raphael Repellin for advanced imaging and surgical expertise.
