December’s Case of the Month-2023
Feline Plasma Cell Tumor in Multiple Locations
Patient Information
Age: 12 years
Gender: Castrated Male
Breed: Domestic Medium Hair Cat
Weight: 11 pounds
History
Presented for abdominal ultrasound to evaluate the underlying cause of anorexia, lethargy, weight loss, and a recent history of diarrhea. A firm, grape-sized nodule was also noted on the top of the patient’s head.
Abdominal Ultrasound Findings
Kidneys: Both kidneys have normal size (Lt/Rt = 3.5/3.6 cm) and normal shape, with coarse, mild to moderately hyperechoic renal cortices that are disproportionately large. There is mild loss of the corticomedullary junction distinction. No pyelectasia seen. A small (0.3 x 0.4 cm) hypoechoic homogenous nodule is present in the left kidney.
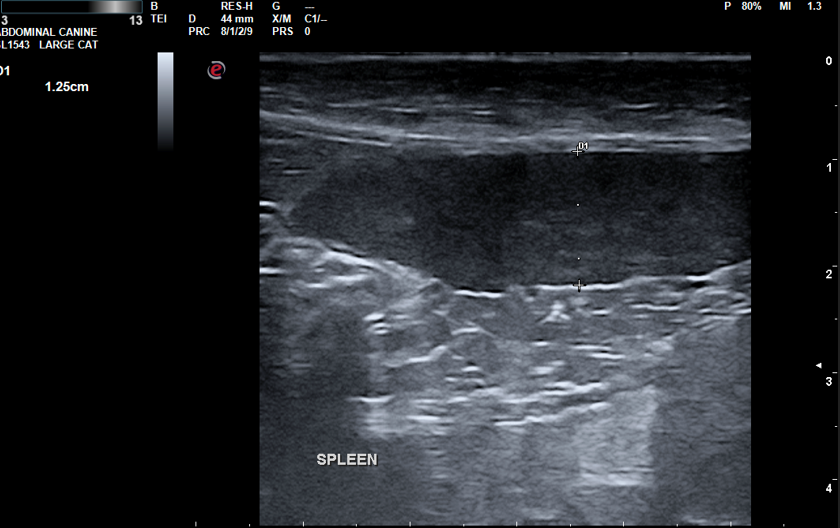
Spleen: Mildly enlarged (1.3 cm depth) with mildly rounded shape and normal echogenicity. No focal lesions appreciated.
Bladder
The bladder is moderately distended with anechoic urine and has a relatively normal contour and thickness. A small 0.3 x 0.2 cm bladder wall nodule is present in the right mid-caudal bladder.
Gastrointestinal Tract
The stomach is empty and collapsed with normal rugal folds and layering. Many loops of intestine are prominent and mildly to moderately thickened (Duodenum 3.1 mm; Jejunum 2.6–3.1 mm; normal wall thickness ~2.2–2.5 mm, >2.8 mm abnormal as per Norsworthy/Estep et al., JAVMA, Vol 243, No. 10, November 15, 2013). Some loops have abnormal layering with prominent disproportionate thickening of the muscularis layer. The colon is mildly thickened (2.0 mm) and has normal layering throughout.
Differentiate Diagnoses
- Splenomegaly: Mild findings. Potential causes include neoplasia (mast cell, lymphoma, carcinoma, metastatic disease), fungal infection (e.g., histoplasmosis), reactive lymphoid hyperplasia, splenitis, congestion, or extramedullary hematopoiesis (EMH).
- Intestines: Potential causes include inflammatory bowel disease or food intolerance, infiltrative neoplasia (small-cell lymphosarcoma or mast cell tumor), parasitism (e.g., cestode), dry FIP, or fungal infection (e.g., histoplasmosis). Chronic inflammatory bowel disease in cats may transition into small-cell lymphosarcoma, but ultrasound alone cannot differentiate between benign and infiltrative disease.
- Inflammation of Large Intestine: Acute colitis/proctitis, chronic colitis (lymphocytic/plasmacytic colitis, eosinophilic enterocolitis, or chronic ulcerative colitis), or IBS.
- Bladder Nodule: Tumors of the urinary bladder are uncommon in dogs and rare in cats. Differential diagnoses include transitional cell carcinoma (TCC), squamous cell carcinoma, leiomyosarcoma, leiomyoma, rhabdomyosarcoma, or benign bladder polyps. Additional differentials: invasion by prostatic neoplasia or metastatic disease (e.g., hemangiosarcoma, lymphoma), bacterial cystitis, urolithiasis, or benign bladder polyps.
Additional Diagnostics
Ultrasound-guided fine needle aspirates of the spleen were obtained for cytology. A fine needle aspirate of the nodule on the head was also performed. Samples of both sites were submitted to Eastern Vet Path for analysis.
Cytology Microscopic Description
Nodule on top of head: Slides are lightly to highly cellular, consisting of red blood cells and nucleated cells. The predominant cells are individual round cells with moderate basophilic cytoplasm, occasional prominent perinuclear clear areas, and eccentric, round to lobulated nuclei. Nuclei exhibit densely clumped chromatin, mild anisokaryosis, rare binucleation, and occasional mitotic figures. See photo below.
Spleen: Slides are of low to high cellularity, with large round cells resembling those in the head nodule predominating. Few small lymphocytes, occasional neutrophils, and rare macrophages are also present.
Comments
For both locations, cytologic findings are consistent with a plasma cell tumor, with 90–100% confidence. If not already performed, consider measuring globulin concentration and serum protein electrophoresis (SPE). Screening the liver and bone marrow may also be considered.

Diagnosis
Nodule on top of head: Plasma cell tumor
Spleen: Plasma cell tumor
Discussion
Unexpectedly, both fine needle aspirates revealed the same disease: plasma cell tumor, suggesting metastatic disease and/or multiple myeloma. Splenomegaly in this patient could have been secondary to sedative medications, as the patient was sedated. The nodule on the head had many other possible differentials. Aspiration of abnormal findings often provides rewarding diagnostic results, even when unexpected.
Outcome
Additional diagnostics recommended for this patient included measuring globulin concentration and serum protein electrophoresis. Screening the liver and bone marrow was also suggested. A referral for oncology consultation and a recheck sonogram to monitor the kidney and bladder nodules was advised. Unfortunately, due to the patient's poor clinical condition and diagnosis of neoplasia, humane euthanasia was performed.
